The South West’s premier independent dermatology & skin clinic

Some supplements for skin, hair, and nail health have been linked to increased risks for birth defects, lab test interference, certain cancer risks, and side effects like acne and hair loss.

Among the most popular supplements believed to help with hair growth and reduce shedding, biotin (vitamin H or B7) is commonly found in foods like eggs, salmon, sweet potatoes, almonds, and milk. High doses can lead to inaccurate lab results, particularly for hormone tests like thyroid levels and troponin, a biomarker used to diagnose heart attacks
Biotin deficiency is rare, and supplements should only be taken if you have a biotin deficiency. Otherwise, they can have adverse effects. No clinical trials currently exist to support claims that biotin supplements improve hair or nail growth or quality.

Strains of good bacteria naturally found in the digestive tract are known for improving gut health. They can enhance skin moisture and smoothness, and help improve common skin conditions like atopic dermatitis, a form of eczema. Yogurt is a good source of probiotics, as are fermented foods like miso, kefir, and fermented vegetables like sauerkraut or kimchi.
Probiotics may have adverse side effects, such as an upset stomach, gas, diarrhoea, or bloating, but these are usually mild and short-lived.

Collagen is available to consumers in both oral and topical formulas, and is often marketed as an anti-aging ingredient, although it may also target those seeking to boost skin recovery and repair. Oral collagen in a hydrolysed form has become popular, but the evidence for efficacy remains mixed.
No adverse events are associated with oral collagen use, although there is a lack of regulation of ingredients in collagen supplements and limited published studies in the medical literature. For example, one cannot be sure collagen from seafood (marine collagen), is free from heavy metals like mercury. High levels of mercury exposure can harm vital organs, leading to kidney damage and cardiovascular issues.
Aging causes a decline in the enzymes involved in processing collagen and a reduction in the number of fibroblasts that synthesise collagen and blood vessels that supply the skin. The decline in skin quality with age is characterised by a reduction in collagen synthesis and a decrease in skin vascularity, leading to decreased elasticity and the formation of wrinkles. The skin undergoes regressive changes with age such as dehydration, a loss of elasticity, and a reduction in epidermal thickness.
Various nutrients and supplements are used to improve skin health and maintain a youthful skin appearance. These strategies include topical creams, injectable fillers, and collagen supplements. Topical creams contain collagen as one of the ingredients, and they are designed to enhance skin hydration and firmness. However, topical creams have limited ability to penetrate the skin, which can reduce their effectiveness – basically ineffective. Injectable fillers such as hyaluronic acid fillers, stimulate collagen production and provide immediate results by plumping and rehydrating the skin. They can be expensive and come with the risk of adverse events such as bruising, swelling, and infection.
On the other hand, collagen supplements, particularly those containing hydrolysed collagen peptides, have been shown to be safe and cost-effective compared to other collagen-based strategies. Furthermore, collagen supplements have the advantage of being taken orally, making them easy to incorporate into daily routines
Collagen is a key protein in our skin, bones, and tendons. As we get older, our body produces less of it, causing a reduction in skin elasticity and the formation of wrinkles. Consuming collagen through food or supplements may improve skin appearance, joint pain, and possibly hair and nail strength.
Marine collagen improves skin hydration and skin elasticity. Chicken derived collagen also improves skin hydration. Bovine collagen appears to be more relevant for muscle mass and joint pain.
Some supplements are available to consumers that stimulate the immune system, especially in those with autoimmune disease. There are laboratory studies that demonstrate the effect of some supplements on activating inflammatory cells, which then produce proteins that further stimulate the immune system. The complete opposite of what is needed when one has an autoimmune condition.
There is increased use of herbal supplements in patients with autoimmune skin diseases. Some patients will experience flares or even new onset of disease in the setting of stating use of these herbs. This has been noted with herbs such as spirulina, green algae, chlorella, ashwagandha, and elderberry.

Most people can get the vitamins and nutrients they need from a well-balanced diet, which can ensure their skin, hair, and nails stay healthy and vibrant.
One trial of multi-ingredient vitamin and mineral supplementation for skin cancer prevention that contained high doses of five antioxidants, including vitamins C, E, and selenium. Unfortunately, after 7.5 years, women taking the supplement had higher rates of skin cancer.
Experts now believe that antioxidants at high doses can become pro-oxidant, but that result was only apparent because this supplement was studied rigorously.
It is the only approved licence medication for this condition.
Alopecia areata is an autoimmune condition that in most case causes mild patchy hair loss that comes and goes. When it is more extensive and widespread it often does not respond to traditional simple treatments such as topical preparations or low strength steroid injections. Up until now, a safe effective treatment for severe and unresponsive cases has not been available..
Oral Ritlecitinib is taken daily at a dose of 50mg a day. A loading dose of 200mg is recommended but not necessary. Hair recovery can take a few months to be seen and continues to improve with long-term use. Patients would be expected to stay on this medication long-term over many years. Common side-effects are headaches, an increased chance of coughs and colds and acne. Patients are recommended to have a Full Blood Count blood test before starting treatment and four weeks into treatment.
There are many different treatable types of hair loss that we routinely manage as Dermatology experts. More information on different types of alopecia/hair loss and this medication can be found on alopecia.org.uk
This medication cost approximately £400 per month privately (excluding consultations and any investigations required).
There is no cure for psoriasis, but there are a number of treatments that can help to control the symptoms. There are many different treatments for psoriasis, including topical creams, light therapy, and oral medications. In some cases, biologics may be used to treat psoriasis. South West Dermatology can offer biological treatment for psoriasis with Dr. Anthony Downs having over 20 years experience in prescribing biologics for patients with moderate to severe psoriasis.
What are biologics?
Biologics are a type of medication that is made from living organisms. Biologics work by targeting specific proteins in the immune system that are involved in the development of psoriasis.
There are many different types of biologics available, and they work in different ways. Some biologics block the production of certain proteins that are involved in inflammation, while others target specific immune cells.
How do biologics work?
Biologics are made from living organisms, such as bacteria or immortal cell lines. They are designed to target specific proteins in the immune system that are involved in the development of psoriasis. By blocking these proteins, biologics can help to reduce inflammation and clear up the skin.
How are biologics used to treat psoriasis?
Biologics are usually given by injection or infusion. The frequency of injections or infusions will vary depending on the type of biologic that you are taking. They can be used alone or in combination with other treatments. Some people see a significant improvement in their psoriasis within a few weeks of starting treatment, while others may not see any improvement.
What are the benefits of biologics?
Biologics can be very effective in treating moderate to severe psoriasis and tend to have fewer side effects than other types of psoriasis treatments. The effectiveness of biologics varies from person to person.
What are the side effects of biologics?
Biologics can be a very effective treatment for psoriasis, but they are not without risks.
Biologics can increase the risk of certain infections, such as tuberculosis and pneumonia. They can also increase the risk of some types of cancer, such as lymphoma.
Are biologics the right psoriasis treatment right for me?
Consultant Dermatologist Dr. Anthony Downs can help you decide if biologic therapy is right for you and look at your own risks and the potential benefits of biologics before starting any treatment. For patients outside the south west area Dr. Downs is able to offer remote video consultations.
What are the costs of biologics?
Biologics can be very expensive. The cost of biologics will vary depending on the type of biologic that you are taking and your insurance coverage you have.
There are many different treatments for psoriasis, including topical creams, light therapy, and oral medications. For some people, these treatments are not effective enough or they cause unwanted side effects. In these cases, biologics may be a good option.
Biologics are a type of medication that works by targeting the immune system. They are typically used to treat moderate to severe psoriasis. Biologics can be very effective in clearing up psoriasis, and they often have fewer side effects than other treatments.
Here are five reasons to consider switching to biologics for psoriasis:
If you are considering switching to biological treatment for psoriasis, talk to Dr. Anthony Downs. Dr. Downs can help you decide if biologics are right for you and make the best decision for your individual needs.
Here are some additional things to consider when deciding whether or not to switch to biologics for psoriasis:
If you have any questions or concerns about biologics, get in touch with us today.
If you feel this is the type of medication for you, then book in a consultation with Dr Anthony Downs. For patients outside the south west area Dr Downs is able to offer remote video consultations
Dr. Anthony Downs has over 20 years experience in prescribing biologics for patients with moderate to severe psoriasis. He has contributed to global clinical trials that have led to these medicines being licenced and continues to be active in clinical research in this field of medicine.
Over 100 people were seen throughout the morning raising money for the Honiton Lions charity that supports many local ventures in and around Honiton and East Devon.

A number of probable melanomas and non-melanoma skin cancers were identified at this event and these will proceed to hospital NHS surgery through their local GPs.
Melanoma is the 7th commonest cancer and Devon and Cornwall has four times the national average.
A big thank you to everyone involved and to all those who attended to support this worthwhile event.
If you have any concerns about your skin or a suspicious mole please get it checked by a medical professional. Look out for a mole which changes progressively in shape, size and/or colour. You can check your moles by learning the ABCDE of moles. This covers a range of features that can help you spot if a mole is becoming cancerous.
Dr. Anthony Downs runs a mole check clinic or you can upload a photo using our online form to get an initial evaluation.
You have been prescribed a course of Isotretinoin for your acne. This information should be read together with the patient information leaflet by the manufacturer of this product.
This is a drug which is used to treat and cure acne. The drug is only available from a Dermatology consultant on prescription. The drug needs to be taken for a specified length of time, which will be explained to you by your doctor.
The capsules should be taken by mouth once a day. Always make sure that you take the capsule on a full stomach and never on an empty stomach.
- Avoid alcohol completely, or only drink small quantities of alcohol, during the treatment course.
- Do not take vitamin A supplements in the form of oral or powder multivitamins.
- Do not take certain prescribed medicines such as Tetracyclines (eg Oxytetracycline, Lymecycline, Doxycycline, Minocycline) or Methotrexate.
Very common side effects include dryness to the face, arms, hair, throat, lips and eyes. The skin is more fragile, so wound and cuts take longer to heal and removing hair by waxing should be avoided.
- You are twice as likely to burn in strong sunshine. This is less of a problem once you have acquired a protective suntan.
- You will not be able to give blood.
- If you are female, you must not become pregnant whilst on this tablet and for 3 months afterward you have stopped the tablet, as you will have a malformed baby and would be strongly recommended to have a termination of the pregnancy. Effective contraception is strongly recommended in fertile women with male partners. Equally men should not attempt to father a child whist on isotretinoin.
- Women’s periods also become irregular on this treatment.
- Skin and nail infections are more common on this treatment.
- Muscles and joints can ache. This is much more likely if you do a lot of exercise, or the older you are when you take this treatment.
- Less common, or rare side-effects include a decrease in night vision, a rise in cholesterol or triglycerides, inflammation of the liver or pancreas, temporary hair thinning, in-growing toe and fingernails and precipitation of gout attack.
- A very rare side-effect, known as benign intra-cranial hypertension, can also occur. This presents with vomiting, a severe early morning headache and blurred vision.
- Inflammatory bowel symptoms can be worsened or triggered.
Your doctor will tell you which side0effects you are more likely to suffer from and which ones are extremely unlikely. If the dosage of tablets is reduced or stopped completely, the side-effects will go away. Make sure you talk to your doctor before making any changes to your medication, if you are suffering from any symptoms.
This can happen to one in ten people that start isotretinoin. The flare is no worse than a flare of your typical acne and settles with 4 weeks. It is not related to your starting dose of medication. Very rarely a severe inflammatory reaction that mimics severe acne can happen. This is usually controlled by adding in oral steroid tablets alongside a reduced dose of isotretinoin.
Because acne causes low self-esteem and depression, it is common to see patients develop depression before or after starting isotretinoin. Unrelated depressive mood changes have been reported after starting isotretinoin. It remains uncertain if these reports are co-incidental or related to the medication. If you have any mood changes, you should report these to your doctor, GP, friends and family.
Very rarely a wide variety of symptoms have been reported including reduced libido. Not many cases have been reported, and only in the last few years. These symptoms can start during or after completing a course of treatment and can persist.
Isotretinoin is contra-indicated in those with a known peanut or soya allergy. Peanuts share proteins with soya. Soya allergy is against soya protein and not soya oil. Isotretinoin capsules contain soya oil. Any soya protein within the capsules is either heavily modified or absent. The risk of having an allergic reaction is therefore theoretical rather than likely. Your doctor may wish to carry out further investigations to establish if you have a Type 1 allergy to peanut or soya and may wish to start your treatment in the clinic rather than at home.
You will need one blood test before you start treatment and at least one blood test approximately six weeks into treatment. It is very rare to require any further blood tests. These blood tests will be 9am fasting samples (no food or drink except for water from 9pm the night before the blood test).
There are no long-term risks of having treatment. All side-effects will go away once the treatment is stopped. The treatment course must be completed in full, otherwise a successful cure of your acne will not happen.
There is a 95% (95 out of 100) chance of you curing your acne with a single course of at least 4 months at a dose of 1mg/kg per body weight per day. Course extensions may be required if you are still spotty after 4 months treatment.
There is a 60% chance of curing your acne if you are older than this.
Lower dosage courses have a reduced chance of curing your acne or not curing you at all.
Please note that isotretinoin is also prescribed by Dermatologists for other types of skin conditions using different dosages and protocols.
There are no known alternative acne cures.
Please tell your doctor if you are on any other medications or supplements before you start treatment, or if you start anything during treatment.
The capsules need to be swallowed whole and cannot be crushed or split open. If you miss your dose that day, do not take a double dose on the next day.
You need to finish all the tablets that have been given to you. By missing a dose, your treatment course will be one day longer.
Store the tablets in a cool, dark place. Keep these capsules away from children.
Your GP cannot prescribe you this drug. This drug is only available from a consultant Dermatologist.
You will be reviewed at least once during your treatment course. Questions and problems can be discussed at this consultation. Most problems regarding this medication can be discussed over the phone or by email.
A wide variety of superficial benign (non-cancerous) lesions can be treated with cryotherapy, but it is most commonly used to remove actinic keratoses (an area of sun-damaged skin found predominantly on sun-exposed parts of the body), viral warts, seborrhoeic keratoses, Bowen’s disease and other benign lesions.
Occasionally, your dermatologist may suggest using cryotherapy to treat a superficial type of a low grade skin cancer known as basal cell carcinoma.
Liquid nitrogen cryotherapy is a traditional Dermatology treatment that is used to remove or destroy superficial skin lesions and blemishes. It takes advantage of the fact that normal skin cells are tougher to destroy and re-grow in the treated area.
Dermatologists have to undergo bespoke training in order to use this treatment correctly and safely. Other freezing techniques, that do not use liquid nitrogen, have not undergone extensive assessment in clinical trials and do not cool the skin sufficiently well enough to make them a reliable or safe alternative.
Training is important to avoid treating a skin problem that should not be treated with liquid nitrogen or avoiding side-effects such as permanent skin scarring, permanent hair loss, nail damage or permanent pale patches. Even with training, there is a risk that these side-effects may happen.
Cryotherapy is a cold burn that feels like a hot burn. It is an uncomfortable but quick treatment. The skin will feel and behave like hot burn afterwards. It will swell, blister, peel and scab. The new skin may stay pink for several weeks afterwards and sometimes temporarily over-darken with sun exposure. The treatment area can be sore or uncomfortable for several days. Daily Vaseline can help soothe this discomfort.
For some skin conditions, there are alternatives to liquid nitrogen that may better suit the situation. Some skin lesions may re-grow after treatment. That does not mean the treatment was not done correctly. It is just that the success rate of treatment is never 100%. Repeat treatments may be required at additional cost.
The cost of cryotherapy is separate and in addition to any initial or follow-up consultation charge. It is not included in the consultation charge. Purchase, storage and compliance with government regulations of liquid nitrogen as well as the skill required to provide this treatment are reflected the the price we charge both for our cryotherapy and consultation charges.
Dr. Anthony Downs, Consultant Dermatologist gave Devon based GPs a skin cancer management update on Thursday 1st July via a virtual lecture hosted by Exeter Medical.
Whist there have been tremendous advances in the last five years in treating and curing patients with melanoma over 50% still die when this disease is advanced. Early recognition and treatment remains essential. The South West has four times the national average of skin cancer.
The COVID pandemic has not helped with patients having to wait a great deal longer for NHS access to surgery by specialist whist their skin cancer continues to grow. Timely intervention by GPs can help reduce the skin cancer burden.
One of the notable differences between the UK and Australia, a country with higher skin cancer rates than the UK, is their lower death rate. This is because Australians proactively undergo routine and sometimes annual full body skin checks with their GP or their Dermatologist. Prevention being preferable to cure.
Full body mole checks are not generally available on the NHS, although your GP will always look at any mole that concerns you. South West Dermatology offer a full body mole check service undertaken by Dr Anthony Downs, Consultant in Dermatology Medicine and Surgery. Dr Downs will make a full assessment of your moles using a dermatoscope.
Dr. Downs is happy to receive a photograph via his online form if you would like an initial opinion on an individual mole.
Dr. Downs is continues to look forward to passing on his knowledge and offering further useful advice and guidance for doctors at the next event.
Dr. Downs recently provided local GPs in Devon with a Zoom based educational session on peri-ocular skin conditions. This professional development session was well attended by local GPs and was some what topical given the current circumstances.
Peri-ocular dermatitis is a common dermatological disorder characterised by inflammation of the eyelids and the skin surrounding the eyes. The cause of peri-ocular dermatitis is not completely understood, but it is thought to be due to a combination of genetic and environmental factors. Peri-ocular dermatitis may be related to an impaired skin barrier – there is an association between atopic dermatitis and peri-ocular dermatitis, disturbance of follicular microflora and/or alteration of the pilosebaceous unit.
There are a number of specific medical and dermatology conditions which need treating or investigation, that present with lumps, bumps or rashes around the eyes.
Equally Dermatologists are adept at providing cosmetic treatments such as lasers for removing blemishes and wrinkles around the delicate structures of the eyes.
Dr. Downs is continues to look forward to passing on his knowledge and offering further useful advice and guidance for doctors at the next event.
Hyperhidrosis - excessive sweating is a common condition that can affect the whole body or just some specific areas. Sometimes excess sweating gets better as you age but there are many things you can do and treatments that can help which are generally explored with your own GP. Excessive sweating can happen for no obvious reason, due to another condition you may have or as a side effect of a drug you are taking.
If you have tried other methods such as: stronger antiperspirants instead of deodorant, armpit or sweat shields, foot powders and soap substitutes and your condition is not getting any better then Botulinum toxin injections can help and may not be available on the NHS.
Botulinum toxin works by blocking the nerves responsible for activating your sweat glands. Normally, your nervous system activates your sweat glands when your body temperature rises. This is how your body automatically cools itself. In people who suffer with hyperhidrosis the nerves that signal the sweat glands are overactive.
Botulinum toxin injections are given directly into the area of your body that commonly sweats, your overactive nerves are essentially paralyzed in this area so that when your nerves can’t signal your sweat glands, you don’t sweat. However, Botulinum toxin only prevents sweating in the specific area where it’s injected.

Studies have found that Botulinum toxin successfully treats sweaty palms in 80 to 90 percent of cases. However, the treatments don’t last quite as long as the underarm treatments. Studies also show that Botox works to treat forehead sweat where it can reduce sweating by 75 percent for about five months.
Researchers believe that Botulinum toxin could help with sweating on the soles of the feet, however few studies have been done. Of particular concern is that injections in the feet are considerably more painful than other areas.

Moles are growths on the skin that are usually brown or black and can appear anywhere on the skin, alone or in groups. Most moles appear in early childhood or during the first 20 years. Some moles might not appear until later in life.
The average adult has around 30 benign moles on their skin. Over time, moles can change, becoming raised and lighter in colour and hairs can also develop on the mole. Some moles will never change, and others will slowly disappear over time.
Any mole that itches, hurts, changes in colour, size, or shape, or bleeds should always be checked by a doctor as these symptoms can indicate the development of a malignant melanoma.

Freckles are small brown spots most commonly found on the face and arms. Freckles can occur in anyone, and appear as darker brown spots in people with darker skin. Both men and women can get freckles.
Freckles do not cause any harm and tend to come out in sunlight and are more prevalent especially amongst pale-skinned people and/or people with light or red hair.

A lentigo or lentigines are spots on the skin that are darker (usually brown in colour) then the surrounding skin tone.
Lentigines more commonly occur in Caucasian patients, in particular those with a fair pale skin, but can also occur in anyone.

Seborrheic keratoses are brown or black growths on the skin most commonly found on the chest and back, as well as on the head. They originate from cells called keratinocytes. As they grow and develop, seborrheic keratoses can take on a wart-like appearance.
The cause of seborrheic keratoses is unknown and they tend to be seen more commonly as people get older. They do not lead to skin cancer.

A skin tag is a small flap of tissue connected by a stalk that hangs off the skin. Skin tags are almost always benign and are not dangerous.
Skin tags tend to appear more in females, especially with weight gain, and in middle-aged and the elderly. They are can be found throughout the body but most commonly on the neck, chest, back, armpits, under the breasts, or in the groin area.
Skin tags are generally not painful but in some cases can become irritated if clothing items, or jewellery rubs and aggravates the skin tag. These can be removed if they are causing discomfort and a full quotation for the surgery and appointment can be made at the time of your skin consultation.
Our Consultant Dermatologist, Dr. Anthony Downs will examine and diagnose any suspicious moles, skin lesions, skin tags or lumps and bumps which are causing you concern. Dr Downs will make a full assessment of your skin condition using a dermatoscope and if any cancerous or pre-cancerous conditions are detected you will be given full information to take to your GP who can arrange treatment on the NHS or, alternatively, you may choose to have treatment at South West Dermatology on a private basis.
If your mole/skin lesion is not suspicious but you would like to have it removed this can be arranged for you, and a full quotation for the surgery and appointment can be made at the time of your skin consultation. The removal of benign moles, skin lesion and skin tags for cosmetic reasons is not currently funded on the NHS.
Suspicious moles & skin lesions consultations can be held at any one of our locations in the South West.
This photographic upload service is designed to help us assess potential patients, check to see if you are suitable to be seen by us, and help you to decide if you would like to book a consultation and what the possible costs may entail. Dr Downs is happy to receive a photograph using the form below if you would like an initial opinion on an individual mole/skin lesion. You can then proceed to book a consultation with Dr. Downs if further investigation is required.
Alternatively fill out the form below for non-urgent enquiries:
On 21 January 2021 Dr. Tony Downs, Consultant Dermatologist was a conference speaker at the national Dermatologists virtual meeting hosted by the Royal Society of Medicine.
Dr. Downs presented on 'Inflammoscopy: no rash or hairy decisions' to a well attended meeting with an audience of over 250 delegates. He presented to fellow consultant colleagues about improving their diagnostic skills enabling them to further their CPD with accreditation.

Other topics discussed at the event were:
The The Royal Society of Medicine (RSM) provides learning and support using expert speakers and global thought leaders providing essential medical insight. The RSM is a membership organisation with over 22,000 members in the UK and internationally. It aims to bringing together doctors and healthcare professionals across specialties, with a vision to be a driving force in advancing health and patient care through education and innovation.
Symptoms are the same in men and women, however around 90% of cases occur in women.
Women of light brown skin types from areas of the world with intense sun exposure tend to be affected more than others. The actual cause of melasma is unknown, but it is known to be related to both hormonal levels and exposure to sunlight. The condition is harmless, but many people with melasma feel self-conscious about the blotches and are dissatisfied with their appearance. In this animation, you will learn the basics of how melasma arises and ways to improve your symptoms or possibly prevent melasma from forming.
Melasma is simply an excessive accumulation of melanin, your skin’s natural pigment, in the skin. People with a family history of melasma are more likely to develop the condition than others. Melasma commonly arises with hormonal changes that occur during pregnancy, and the term chloasma is used synonymously with melasma for the condition among pregnant women. This onset of melasma often disappears shortly after childbirth, but it may remain for months, years, or a lifetime. Melasma is also known to arise among women taking hormonal birth control pills, and it sometimes occurs in women taking progesterone hormone replacement therapies following menopause. Certain medications as well as facial cleansers, creams, and types of makeup that irritate the skin may cause or worsen melasma.

Your skin is made of two primary layers; the epidermis is the surface, and the dermis lies beneath it. Located near the base of the epidermis are specialized cells, called melanocytes, which produce the pigment melanin. Melanin gives your skin its normal color, and it is transported into new skin cells where it serves a protective role by absorbing harmful rays of sunlight that would otherwise damage the cells. When melasma occurs, melanocytes in certain areas overproduce melanin. As accumulating melanin gradually becomes more visible, the characteristic patches occur. The excessive melanin typically exists near the base of the epidermis, and appears as tan or brown blotches. However, the pigment may also be associated with cells near the top and mid-dermis, in which case, blotches can appear from light brown to bluish black.
Melasma tends to worsen with increased sun exposure. The best method for preventing melasma from forming, worsening, or recurring is strict sun avoidance. Daily use of a broad spectrum sunscreen of SPF 30 or greater that blocks both the UVA and UVB forms of light is recommended. Sunscreens that use metallic compounds, such as titanium oxide or zinc oxide, to block, rather than absorb ultraviolet light may be the most effective when spending time outdoors. Full-length clothes and a wide brimmed hat also help minimize sun exposure. It is paramount to strictly avoid sun exposure, even following treatment, because even incidental sun exposure may cause a recurrence. If possible, discontinuing certain medications, cleansers, creams, or makeup suspected of irritating your skin or making your melasma worse may improve your symptoms. If melasma is caused by the birth control pill, discontinuing the pill may cause it to clear and prevent future occurrence. When discontinuing a certain product, it’s important to keep in mind that just as melasma tends to arise gradually, it also tends to clear very gradually.
Melasma cannot be cured permanently, but various treatments options may help clear the patches. The principal treatments are topical depigmenting creams containing hydroquinone, which decreases the activity of melanocytes without destroying them. Azelaic acid is also used topically, and is believed to inhibit melanin production in overactive melanocytes. For people who aren’t pregnant, topical treatments with tretinoin are sometimes used. Trentinoin is believed to increase the turnover of cells that accumulate excess melanin, thus allowing pigment to be cleared as the cells die. Other treatments, including chemical peels and laser treatments, are used by some skin care professionals to physically remove the pigment. These treatments are often used in conjunction with topical treatments. Keep in mind that treating melasma can take several months, and some treatments will work better for certain people than others. Discuss your specific situation with a skin care professional to find the treatment option that will be the safest and most effective method for you.
Fortunately, it is a self-limited skin infection, meaning it will disappear spontaneously, without specific treatment. Although this is the case, a single molluscum contagiosum papule may take from three months to two years to disappear. For this reason, many people may prefer to eliminate the infection as soon as possible and seek treatment, since molluscum contagiosum may cause physical or emotional discomfort and can be spread.

Papules appear on your skin when the molluscum contagiosum virus successfully reproduces within your skin cells. The virus can enter your body through pores, hair follicles, or through abrasions on the skin surface. The virus then inserts part of itself into your skin, where it is replicated many times. This causes the skin cells to swell and rupture, creating raised, pearly, skin-colored papules on the skin surface with an infectious virus-containing core at the center. If a papule is scratched or picked, the infectious central core is released and can be spread to whatever is subsequently touched, including uninfected areas of the body or other people. Rarely, transmission can occur when objects that an infected person has touched come in contact with an uninfected area or person.
Molluscum contagiosum can appear anywhere on your body, although it rarely affects the palms of the hands and the soles of the feet. This condition occurs most frequently in children between the ages of one and ten, in sexually active adults, and in individuals with a compromised immune system. In children, molluscum contagiosum commonly occurs on exposed areas of skin such as the face, trunk, arms, and legs. In sexually active adults, this infection is typically found on the lower abdomen, buttocks, groin, genitals, and inner thighs. In individuals with a compromised immune system, molluscum contagiosum frequently occurs on the face as well as in the genital region.
If you are infected with molluscum contagiosum, it is important to take precautions to avoid spreading it to uninfected areas of your skin or to other people. If you anticipate contact with other people, all areas infected by the virus should be covered by a bandage or clothing. Your clothing, towels, and personal items should not be shared with others. Papules should not be scratched, picked, or touched, and in the case that they are, you should wash your hands immediately and thoroughly. In addition, shaving any infected areas should be strictly avoided. If the molluscum contagiosum infection affects your genital region, sexual activity should be avoided until after all papules have cleared.
To effectively treat molluscum contagiosum, the infectious, virus-containing core at the center of each papule must be destroyed. Once the core of each papule is eliminated, the infection will subside and the virus can no longer be spread. The virus-containing cores can be destroyed by various treatments. A curette, scalpel, or other cutting device can be used to surgically remove the papules. Infected individuals can also undergo cryotherapy, in which a substance, such as liquid nitrogen, is applied to the papules to freeze and destroy the infected cells. Pulsed dye lasers can be used to target and destroy infected cells with light energy. Additionally, a variety of astringent chemical agents such a podophyllin, cantharidin, or trichloroacetic acid can be used to destroy layers of skin containing the cells infected with the molluscum contagiosum virus. The virus-packed cores are eliminated when the dead skin sloughs off, and healthy, virus-free skin grows back in its place.
Although molluscum contagiosum can be unsightly or uncomfortable, this infection is not life-threatening. However, because it is contagious, precautions must be taken to avoid spreading the infectious virus to other parts of the body or other people. For those who prefer to eliminate the infection before it resolves on its own, several treatment options are available. Consult your physician to find the best treatment option to fit your particular needs.
It commonly occurs on and around the nose, cheeks, forehead, chin, eyelids, and occasionally on the neck and upper chest. The redness sometimes progresses to visible vessels; swollen bumps, called papules, or pus-filled bumps, called pustules, that are often mistaken for adult acne; and in some cases, thickened skin that results in a red, bulbous nose. Most people with rosacea don’t even realize they have it and are not treating it. Although the red facial skin is harmless, the red-faced appearance often causes people with rosacea to be unhappy with their appearance.

Rosacea results from a cascade of events starting with skin inflammation that causes blood vessels to dilate. The enlarged vessels also become more permeable and leak white blood cells into the surrounding, inflamed connective tissues. The white blood cells within the connective tissue cause swelling and also stimulate the growth of additional blood vessels, some of which grow near the surface of the skin and become visible. Over time, the new vessels will dilate and become more permeable, continuing the cycle. The dilated vessels cause the telltale redness associated with rosacea. Although some people describe being able to see broken vessels with certain stages of rosacea, they are generally referring to the visible, enlarged vessels near the skin surface.
Before learning about rosacea treatment and prevention, it will help to understand a little about your skin and how rosacea occurs. The skin is composed of two main layers: the epidermis and the dermis. The epidermis is the outer layer that acts as the body’s primary defense against the environment. The inner layer, or dermis, is comprised primarily of connective tissue, which is made mostly of collagen and elastin fibers. These fibers form a network that provides your skin with structure, support, and elasticity. Rosacea develops as a result of skin inflammation, changes to the skin’s connective tissue, and dilation of the blood vessels in the dermis.
Scientists do not fully understand what causes rosacea. Rosacea may arise from a single specific trigger, or as a result of a combination of factors and genetics. There is evidence that certain environmental factors, foods, drinks, and medications may trigger rosacea. In addition, some researchers believe that specific living organisms may possibly even play a role in the flushing and blushing that precede rosacea.
Rosacea affects people of all ethnicities, skin colors, gender, and age. However, there are patterns in which certain groups of people are more likely to develop rosacea than others. Rosacea tends to occur in fair-skinned people more often than people with darker skin. The onset of rosacea primarily occurs between the ages of thirty and sixty, but it can also first appear in children or the elderly. Rosacea afflicts many more women than men, and it is sometimes occurs around menopause. However, although there are more cases in women, men generally develop far more severe rosacea symptoms.
Rosacea doesn’t always worsen over time, but the symptoms tend to progress when left untreated. As rosacea progresses, it may present symptoms from any or all of four different subtypes. Based on genetics, some rosacea sufferers are more susceptible to certain symptoms than others. Early diagnosis and treatment is often effective in preventing the progression of rosacea symptoms. Therefore, if blushing tends to be brought on by your diet, medications, or other environmental factors; or if you notice that periods of flushing last longer and longer, consult your dermatologist.
A dermatologist can help you identify substances or activities that cause flushing and trigger rosacea flare-ups. Keeping a symptom diary may also help to see patterns and identify triggers that make your rosacea worse. The best prevention is to avoid triggers. If you find that you are sensitive to sun exposure, specific skin care products, foods, drinks, alcohol, tobacco products, stressful situations, temperature extremes, or strenuous exercise, do your best to avoid them. Your dermatologist may recommend a regimen that includes using mild cleansers or warm compresses or may even provide prescriptions for various acne products, medications that inhibit immune reactions, antibiotics, anti-inflammatory medications, or cell-growth inhibitors, based on your needs. Additionally, laser procedures can be effective in removing tissue growth or reducing the redness and visible vessels once rosacea triggers are under control and symptoms subside.
Rosacea responds to treatment, but it may take several weeks or months before you notice improvement. Papules and pustules generally respond to treatment quickly; whereas redness and flushing tend to respond slowly. Be patient, as your dermatologist may need to tailor your medication dosages or suggested skin care routines to achieve the desired results for your particular needs. By following the customized treatment plan and avoiding triggers, you can often stop the progression of rosacea over time and even reduce your symptoms and improve your skin’s overall appearance.
Vascular IPL at Exeter Medical is an effective way of managing some rosacea symptoms. It can remove fixed red patches or thread veins on the face. It reduces prolonged flushing and blushing and skin burning. It reduces skin sensitivity to facial products or changes in temperature. It can be very useful in managing the debilitating but thankful less common painful neurogenic rosacea.
One of these warning signs is actinic keratosis (AK)—a skin condition that is believed to be a precursor to certain types of skin cancer. Although generally harmless, actinic keratosis may be the first sign of a more serious medical condition, which is why it is important that you examine your skin on a regular basis and seek medical advice and treatment should you identify any irregularities in your skin.
Before you understand what actinic keratosis is and how to identify it, it is important that you understand its underlying cause. While actinic keratosis can be caused by carcinogens, or cancer-causing agents, like exposure to radiation and chemicals, the most common cause of actinic keratosis is exposure to ultraviolet light produced by the sun. Much like squamous and basal cell carcinoma, actinic keratosis is generally caused by long-term, cumulative sun exposure. This is why actinic keratosis is often referred to as solar keratosis. Ultraviolet light damages the DNA of epidermal skin cells, which causes them to develop abnormalities in size, shape, and organization. These changes may cause the cells to divide uncontrollably, resulting in a lesion or plaque on the skin’s surface. Left untreated, the damaged cells can become cancerous with time.

Just as certain individuals are at a higher risk for developing sunburn than others, some people are at a higher risk for developing actinic keratosis. In general, those with fair skin and blond or red hair develop actinic keratosis at a higher rate than those individuals with darker complexions. Because actinic keratosis is primarily linked to sun exposure, people who live in sunny areas or who spend a significant amount of time in the sun without proper protection are also at a higher risk of developing the condition. DNA damage that occurs from occasional sun exposure is usually repaired by built-in DNA repair mechanisms in your body. However, long-term sun exposure can lead to DNA damage that is not repaired. This is why the effects of sun damage are not usually evident for many years, and why actinic keratosis is most commonly observed after the age of forty.
As actinic keratosis generally develops in areas of the body that have been exposed to large amounts of sun, the condition is most often seen on the face, ears, neck, lips, forearms, and hands. Actinic keratoses appear as rough, callous, scaly lesions or plaques on the skin’s surface. Although dry, rough patches are characteristic, actinic keratoses may also present as oozing lesions that do not heal or as thick, horny growths. Lesions may vary in color from light beige tones to dark brown and range in size from a small dot to approximately an inch in diameter. In addition, they may seem to appear and disappear periodically, or they may remain in place for a long period of time. Actinic keratosis can look remarkably like certain types of skin cancer—particularly squamous cell carcinoma. This is why it is important that you contact a dermatologist to determine the nature of any suspicious lesion on your skin.
Aside from being unsightly, actinic keratosis can lead to the development of skin cancer—predominantly squamous cell carcinoma. Therefore, although the lesions themselves are not cancerous, it is important that you take measures to prevent actinic keratosis. Clearly, the best line of defense is to avoid sun exposure. In general, you should avoid being in the sun from 10 AM to 2 PM as the sun’s rays are at their most intense during this time. Even on a cloudy day, dermatologists recommend applying a daily broad spectrum UVA and UVB sunscreen of SPF 15 or greater to protect your skin from incidental exposure. Lastly, wide-brimmed hats, long-sleeved shirts, and long pants provide excellent sun protection.
A dermatologist will usually be able to diagnose actinic keratosis during a skin examination. However, large, thick or otherwise questionable lesions sometimes require a small sample, called a skin biopsy, to be taken to ensure that it has not become skin cancer. Not all types of keratoses need to be removed, but you should consult with a dermatologist, who will make a determination based on the type of lesion, your health condition, and age. Fortunately, there are a variety of treatments.
Our Consultant Dermatologist offer whole body mole checks and skin cancer identification with dermoscopy and treatment with skin cancer surgery. We also offer photodynamic Therapy for pre-malignant lesions and early skin cancers.
Age spots are also known as solar lentigines, sun spots, liver spots, and freckles. They are a result of sun exposure over time, and therefore they become more common as one ages. In this animation you will learn the symptoms and causes of age spots, ways to limit them from forming, and methods for removing or lightening them once they’ve formed.
Age spots are flat, tan, brown, or black flat spots that are darker than the surrounding skin. Age spots, which are called lentigines, differ from another type of light tan freckles, called ephelides, that disappear or fade after seasonal sun exposure. Age spots are permanent freckles that generally tend to arise after around age 40 and occur most frequently on areas that receive the most sun exposure. Age spots are simply a concentrated region of your skin’s natural pigment, and it is not essential to treat or remove them. However, although age spots are harmless, certain forms of skin cancer can start out resembling them. Any new or questionable spot, especially any freckle that changes appearance, grows, or causes discomfort, should be examined by a dermatologist

Your skin is made of two primary layers; the epidermis is the surface, and the dermis lies beneath it. Located near the base of the epidermis are specialized cells, called melanocytes, which produce the pigment melanin. Melanin gives your skin its normal color, and it is transported into new skin cells where it serves a protective role by absorbing harmful rays of sunlight that would otherwise damage the cells. The body actually produces extra melanin in response to sun exposure, and this is why you tan in the sun. However, after years of sun exposure, melanocytes in certain areas of the skin may overproduce melanin. As accumulating melanin gradually becomes more visible, an age spot develops. Genetics also influences how likely a person is to develop age spots.
Preventing Age Spots
Although age spots are a natural occurrence related to your lifetime sun exposure, they are also rough indicators of aging, and many people would rather avoid developing them. Avoiding unnecessary sun exposure is the best prevention. Using a daily sunscreen of SPF 15 or greater that protects against two forms of ultraviolet light: UVA and UVB is also recommended. Certain sunscreens that use metallic compounds, such as titanium oxide and zinc oxide, to block, rather than absorb ultraviolet light may be the most effective at preventing sun damage. Unfortunately, age spots result from past sun exposure so even taking preventative steps now won’t prevent all new age spots from forming. However avoiding sun exposure and protecting yourself with sunscreen also greatly reduces your chance of developing skin cancer.
Age spots that have formed won’t disappear without treatment. Fortunately, there are several ways to treat age spots: topical skin treatments, physical removal, and light treatments and laser. Consulting with a skin care provider will help you determine the specific treatment type and method to suit your particular need for treatment time, cost, and recovery. To view examples of types of treatments that can improve your age spots, roll over any of the treatment types on your screen.
During your consultation you will be given an indication of the number of treatments required and at this stage may require a patch test. Subsequent treatments will take place every 6-8 weeks.
In other instances, individuals wish to lessen the need for shaving, waxing, tweezing, or other methods of hair removal. Most commonly, laser hair removal is used to reduce hair growth on the face, back, legs, forearm, underarm, and bikini line. However, laser hair removal can be used to permanently reduce the amount of hair on any area of the body.
Before you learn how laser hair removal works, you need to understand how hair grows. Hair grows from deep within hair follicles, which are thin cavities embedded in the dermis. Hair does not grow continuously, but grows in a three-phase cycle. While the rate at which hair grows differs by individual, the length of the hair growth cycle generally depends on the type of hair. For example, the active growth phase of the hair on your head may last several years, while hair on the body has an active growth phase that may last only a few months.
Each growth cycle includes an anagen, catagen, and telogen phase. During the anagen phase, the hair grows actively from the follicle. The next phase of the growth cycle is the catagen phase. This is a short transitional period in which the hair stops growing and the hair follicle shrinks in size. The follicle breaks away from the dermal papilla, which supplies nutrients to the hair follicle. The dermal papilla then regresses. The last phase of the growth cycle is the telogen, or resting phase. During the telogen phase, the hair follicle reattaches to the dermal papilla, at which point the follicle re-enters the anagen phase. As a new hair begins to grow, the old hair is pushed out of the follicle.
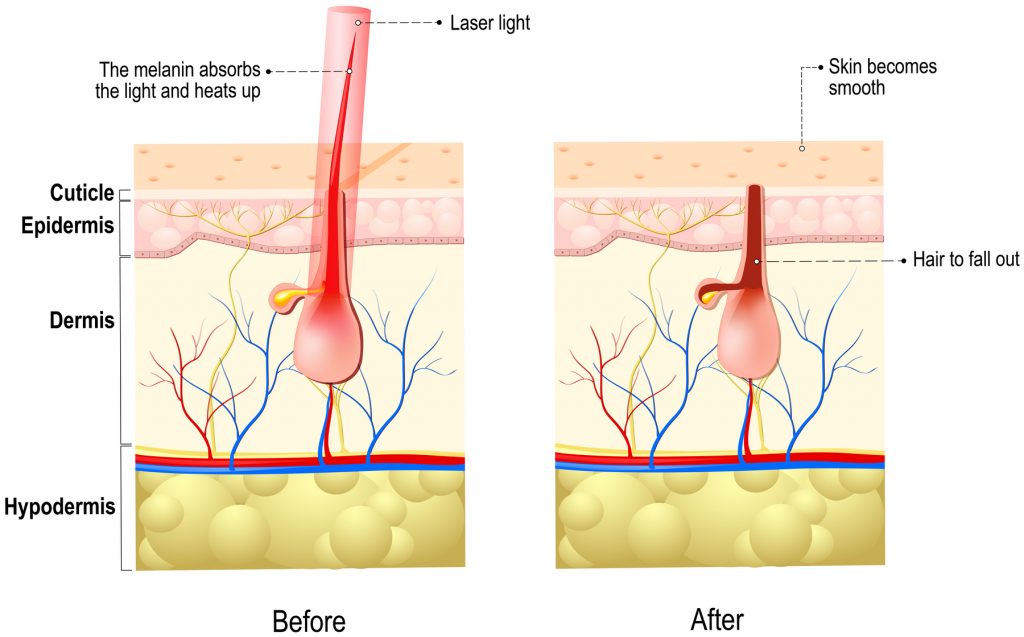
During laser hair removal, a laser emits light energy that travels through the skin and is absorbed by the pigment in the hair follicle and hair shaft. Pigments are the substances that give skin and hair its color. The laser works by selective photothermolysis, which means that the light energy is selectively absorbed by pigmented areas. Hair follicles that are in the anagen, or active growth phase, have the largest amount of melanin, or pigment, and can absorb light energy from the laser. However, hair follicles that are in catagen or telogen growth phases are less pigmented. Therefore, these follicles do not absorb light energy as well and hair growth is not impaired. The energy, or heat, from the laser damages the hair follicle, which impairs its ability to grow hair. With time, the hairs that were present in the damaged follicles will fall out, resulting in a smoother appearance and less hair growth.
It is important to realize that light energy will be absorbed by any type of pigment. For optimal results, your hair must be darker than your skin. This is why individuals with fair complexions and dark hair are better candidates for laser hair removal than individuals with darker complexions or lighter colored hair. If you have a darker complexion, the pigment in your skin will absorb some of the light energy emitted from the laser. As a result, the hair follicles may absorb less energy and your skin may be damaged by the laser. In these instances, your physician may choose to use a lower laser setting, which emits less energy. If you have lighter colored hair, your hair follicles have less pigment. Therefore, the follicles will not absorb energy from the laser as well as those with darker pigment. In both of these instances, it is likely that you will require more treatments to achieve the desired outcome. However, with new technology, laser hair removal may be used successfully on individuals of all skin and hair types.
Prior to the start of your procedure, the physician may choose to shave or trim the hair in the area. Often, the physician will apply a cooling gel to the treatment area, which will help prevent heat produced by the laser from damaging your skin. In contrast, the physician may use a laser with a special cooling tip that applies a coolant during the procedure. Although the procedure is not typically painful, you may request a topical anesthetic if you are especially sensitive to pain. You will likely be given eyewear to protect your eyes from the intense light produced by the laser. The length of a laser hair removal procedure depends on the treatment area. A procedure in which hair is removed from a small region, such as the underarm, may take only minutes, while a larger area, such as the legs, may last approximately one hour.
During the procedure, the physician will guide the laser over the treatment area. As the laser pulses intermittently, it delivers light energy, which travels through the skin and is absorbed by the hair follicles. Hair follicles in the anagen growth phase have more pigment than follicles in the other inactive phases of the growth cycle. Therefore, they are able to absorb the light energy delivered by the laser. Those hair follicles that absorb energy, or heat, from the laser will be damaged. Hairs that were present in the follicles at the time of treatment will fall out, and future hair growth will be impaired. As not all hairs are actively growing at the same time, a single procedure will not treat all of the hair follicles in the area. As the follicles in the transitional and resting periods return to the active growth phase, you may notice some hair growth in the region. This is why multiple treatments are usually required to treat a single area completely.
Following the procedure, your skin may appear red or irritated. However, the redness will likely dissipate within one to two days. Your physician may recommend that you use a topical cream to protect your skin as it heals. It is also important to use sunscreen for a few weeks following the procedure. You should not use any products that may irritate your skin such as alpha hydroxy acids or harsh astringents. In addition, you should avoid plucking or waxing of the treatment area.
You may notice some hair that appears on the surface of your skin within seven to ten days following treatment. These hairs are usually those that have fallen out of hair follicles impaired during treatment. However, you will notice some new hair growth within a few weeks, as hair follicles that were inactive during treatment re-enter the active growth phase. Therefore, you will most likely undergo multiple treatments spaced approximately four to eight weeks apart. Although the number of treatments varies by individual, most individuals receive approximately six to eight treatments.
The results from a laser hair removal procedure depend on your skin tone, your hair type, and the growth phase of the hair being treated. It is important to realize that laser hair removal will likely not prevent hair from growing completely.
However, laser hair removal can reduce hair growth significantly over time giving your skin the smooth appearance that you desire.
Exeter Medical use both IPL and Diode hair removal. In-motion diode hair removal is very effective and a lot less painful than traditional single discharge lasers or IPLs.
There are many different machines that offer a similar type of treatment. We chose our machine (the Youlaser) because it delivers two laser beams into the skin at different wavelengths. It was a significant advancement in treatment five years ago when we purchased this device.
The CO2 laser vaporises the skin and a second 1540nm laser heats underneath the skin. The combination allows for much safer re-organisation and healing of the skin at lower energy settings compared to other fractionating devices. This reduces patient risk and discomfort without compromising on effectiveness.
The 'down-time' is approximately five days. There is minimal treatment and post-treatment discomfort. We will give you advice how to care for your skin after treatment. This laser treatment is an outpatient procedure and can take up to 60 minutes to complete. Risks are low and repeat treatments can improve on any benefit achieved. The commonest treatments we treat are:
The light emitted from Ipulse helps to destroy the bacteria which causes acne by exciting the existing oxygen molcules and increasing the molecules power. These super powered molecules break down the bacteria that cause acne and create an atmosphere where it cannot breathe. By boosing the skin’s internal cleansing system in this way, Ipulse dramatically reduces acne and the occurrence and apperance of scarring, resulting in much clearer skin.
It can often be difficult to assess suitability for Fractionating CO2 laser for acne scarring and facial rejuvenation.
Our Fractional CO2 service is run at Exeter Medical.
Some types of fungus such as moulds, however, do not respond to tablet treatment. The tablets commonly cause side-effects and for some people require blood test monitoring in case of drug-induced liver inflammation.

Initial assessment is by our laser practitioner. Onward private referral to a dermatologist or back to your GP may be required if the diagnosis is not nail fungal infection.
It is the responsibility of the client to remove his or her own nail varnish completely before booking an assessment or treatment appointment.
A laser treatment course of 4 treatments (one each week) has over an 80% success rate and several nails can be treated at each treatment session. We can also provide you with advice to prevent re-infection.
Laser treatment available at Exeter Medical only. Other treatment options include topical anti-fungal and tablet treatments. A consultation may be required to work out what is best for you.
Whole body dermoscopy increases sensitivity and specificity of melanoma diagnosis. Fewer harmless lesions are unnecessarily removed and early melanomas that would otherwise have been missed by simple visual inspection are identified.
We all enjoy sunshine and sunlight is our main source of vitamin D, which is vital for good health.
However, excessive exposure to sunlight over the years can damage the skin. This can result in prematurely aged or wrinkled skin and, of course, a variety of skin cancers.
Full body mole checks are not generally available on the NHS, although your GP will always look at any mole that concerns you.
South West Dermatology offer a full body mole check service undertaken by Dr Anthony Downs, Consultant in Dermatology Medicine and Surgery. Dr Downs will make a full assessment of your moles using a dermatoscope.
Mole Removal

If any cancerous or pre-cancerous moles are detected you will be given full information to take to your GP who can arrange treatment on the NHS or, alternatively, you may choose to have treatment at South West Dermatology on a private basis.
If a mole is not suspicious but you would like to have it removed anywaythis can be arranged for you, and a full quotation for the surgery and appointment can be made at the time of the mole check. The removal of benign moles for cosmetic reasons is not currently funded on the NHS.
The average adult has around 30 benign moles on their skin, but any mole that itches, hurts, changes in colour, size, or shape, or bleeds should always be checked by a doctor as these symptoms can indicate the development of a malignant melanoma.
Each year, 2 to 3 million non-melanoma cancer patients, and 132,000 melanoma patients, are diagnosed globally. When prevention fails, catching skin cancer early is crucial and highly treatable.
A group of young creatives in Vienna realized by their own experiences with skin cancer, that there’s not much knowledge about these type of cancers and so they decided to raise awareness of melanoma and other skin cancers, and encourage self-exams for early detection by starting an online campaign called “Spot the Dot”. Visit www.spotthedot.org for more info.
If you have experienced a lot of sun exposure in the past, especially sunburn, and have one or more moles on your body that you would like to have looked at, a full body mole check may be worth considering.
The mole check clinic is held at Exeter Medical at the Exeter Business Park and Mount Stuart Hospital in Torquay.
A cancerous or pre-cancerous mole could possibly be detected even before you notice it yourself and a treatment plan put in place.
* Mole/lesion checks are £180 and a standard consultation which can include a mole check is £250. Make sure you book the correct consultation for you.
This photographic upload service is designed to help us assess potential patients, check to see if you are suitable to be seen by us, and help you to decide if you would like to book a consultation and what the possible costs may entail. Dr Downs is happy to receive a photograph using the form below if you would like an initial opinion on an individual mole/skin lesion. You can then proceed to book a consultation with Dr. Downs if further investigation is required.
If you need to book an urgent consultation then please phone 01392 350059 (Exeter) or 07421 022801 (Truro).
Alternatively fill out the form below for non-urgent enquiries:
The full body mole check clinic including any pre-consultation photographic triage, is led by Dr Anthony Downs acting in a private capacity as an agent of South West Clinical Dermatology Ltd. Full liability for the opinions expressed & treatments received rests with South West Clinical Dermatology Ltd, or with other Consultants offering private services within the context of the mole check clinic, and not with Exeter Medical Ltd.
Skin cancer is rarely lethal, with an extremely high recovery rate when diagnosed early. Even more important, because most types of skin cancer have been linked to long-term sun exposure, you can take steps to reduce the likelihood that you will be diagnosed with skin cancer. In this animation, you will learn not only what skin cancer is and how it develops, but also what you can do to prevent it as well as the treatment options available to those who have been diagnosed.
The cells in your body continuously divide, or proliferate, in order to grow as well as repair or replace damaged cells in the body. Cell division is a highly regulated process. So what regulates these cells? Specific genes, which are coded in your DNA, are responsible for controlling cell division by communicating when to start and stop dividing. If the DNA that makes up these genes is damaged, or mutated, and not repaired properly, the genes may not function correctly. In some cases, DNA damage to a gene that controls cell division may cause a cell to divide uncontrollably. When this happens, a tumor develops. It is important to realize that not all tumors are cancerous. Benign tumors are generally localized to a specific area and do not invade surrounding tissue. In contrast, cancerous tumors invade surrounding tissues and can metastasize, or spread, to other areas of the body.
Now that you have a general idea of what cancer is and what causes it, let’s take a look at how skin cancer develops. Like other types of cancer, skin cancer often starts with DNA damage. DNA damage can be caused by many different carcinogens, but UV radiation from the sun causes most of the damage that eventually leads to skin cancer. Damage that occurs due to occasional sun exposure is usually repaired by built-in DNA repair mechanisms in your body. But, long-term sun exposure can lead to DNA damage that is not repaired. If this damage occurs in genes that are responsible for controlling the division of skin cells, these cells may begin to divide uncontrollably, which can result in skin cancer.

Skin cancer typically affects three different types of cells in the epidermis, known squamous cells, basal cells, and melanocytes. Squamous cells are cells that have flattened as they progress from the basal cell layer toward the skin’s surface, where they are shed. Basal cells are the bottommost epidermal cells that lie along the junction between the epidermis and dermis. As these cells divide, they produce new cells that eventually become squamous cells, which constantly replace the dead skin cells that are shed at the skin’s surface. Melanocytes are a special type of cell located in the basal layer of the epidermis. These cells are responsible for producing melanin, or pigment, which gives your skin and hair its color.

There are often warning signs that can indicate that you are at risk for developing skin cancer. One of these signs is the development of actinic keratosis. Actinic keratosis may be difficult to distinguish from skin cancer, but is typically easily treated if diagnosed early. Most common in people who are forty or older, actinic keratoses are generally caused by long-term exposure to ultraviolet light from the sun. Ultraviolet light damages epidermal skin cells, which causes them to develop abnormal characteristics. While these changes do not cause the cells to become cancerous, they are considered precursors to skin cancer. Much like skin cancer, actinic keratoses generally develop in areas that have been exposed to large amounts of sun such as the face, neck, ears, lips, forearms, and hands. Actinic keratoses appear as rough, callous lesions, and vary in color from light beige tones to dark brown and range in size from a small dot to approximately an inch in diameter.

Accounting for more than eighty percent of diagnosed cases in the United States, basal cell carcinoma is the most common form of skin cancer. Basal cell carcinoma originates in basal cells and typically does not grow very rapidly. Basal cell carcinoma tumors usually grow in a localized area and do not spread to other areas of the body. However, early detection and treatment will prevent the tumor from spreading into surrounding tissue and causing more damage. Scientists believe that this form of cancer is primarily caused by long-term sun exposure; therefore it most commonly occurs on sun-exposed areas such as the face, ears, head, and chest. Basal cell carcinomas can take on a variety of different forms, appearing as shiny bumps, wounds that will not heal, or even red, irritated growths.

Squamous cell carcinoma is the second most common form of skin cancer in the United States, accounting for less than twenty percent of skin cancer diagnoses. Squamous cell carcinoma originates in squamous cells, and like basal cell carcinoma has been linked to long-term, cumulative sun exposure. This type of cancer is more likely to metastasize, or spread, to other areas of the body through the lymph nodes or bloodstream than basal cell carcinoma, making it more difficult to treat and possibly lethal. However, with early detection, treatments are typically very successful. Like basal cell carcinoma, this form of cancer is most commonly found on sun-exposed areas such as the face, ears, head, and chest. Approximately one inch in diameter, squamous cell carcinoma can look like a red, scaly lesion, wart-like bump, or a wound that does not heal.

Although melanoma accounts for fewer than five percent of the skin cancer diagnoses, it is the most lethal form of skin cancer. However, even this aggressive form of cancer can be treated successfully if diagnosed early. Unlike non-melanoma skin cancers, which are generally linked to the effects of long-term sun exposure, melanoma has been associated with periods of intense sun exposure such as sunburn. In addition, research has shown that certain genetic variants can contribute to melanoma. This form of skin cancer originates in melanocytes and can metastasize, or spread, to other areas of the body, making it more lethal than other types. Melanoma may first appear as a mole on the back, legs, hands, fingers, soles of feet and toes, and the mucous membranes that line the nose and mouth.Step 9: PreventionUltraviolet light plays a critical role in the development of skin cancer, and therefore protecting yourself from the sun is the best preventative step you can take. Avoid unnecessary sun exposure, and protect yourself by covering up with long sleeved shirts, pants, and wide brimmed hats when possible. If your skin will be exposed, dermatologists recommend a SPF 15 or higher sunscreen that protects against both UVA and UVB forms of sunlight.
For the scar free treatment of thin skin cancer and pre-cancerous growths where surgery would be disfiguring
Photo Dynamic Therapy (PDT) for thin skin cancers and pre-cancerous skin growths
Porphyrins are naturally occurring chemicals that when exposed to light glow or burn. This phenomenon has been exploited to successfully treat many different kinds of cancer.
Skin cancers which are confined to the epidermis (upper skin layers) and pre-cancer growths (those that will eventually become skin cancers) can be treated very successfully with PDT. These types of tumours and growths tend to be thin but large. To remove them surgically is complicated and often requires a disfiguring skin graft. Surgery is not always successful because of the tendency of these lesions to form discrete satellite clusters.
PDT is a recognised treatment for:-
How does PDT work?
The porphyrin chemical is absorbed by abnormal cells only. Natural light is shone onto the skin either at a high dose over a short time or at a low dose over a longer time period. Two treatments are required separated by at least two weeks.
How is the treatment carried out?
You will be asked to attend the clinic a minimum of 3 hours before hand. At this time the porphyrin containing cream will be applied to the skin to be treated and then covered. After 3 hours, the cream is wiped off and natural light is shone onto the skin with either a halogen light source (approx 9 mins) or an IPL device (approx 1 min).
Am I suitable for treatment?
There are no contra-indications except pregnancy and a few rare skin and liver disorders. If a scar free result is important to you, then you should seriously consider PDT.
Is it safe?
The treatment is uncomfortable when the light is being shone onto the skin. The skin will have the appearance of a graze or sunburn after treatment and slowly settle back to a normal flesh colour. Any blotchiness or freckles will also be removed from the treated area.
How many treatments are necessary?
Two – one treatment each week.
Aftercare
Avoid sun exposure on the treated area and keep it dry for 24hrs.
For Exeter call Ros on 07838 293968
A patch test can help us find the cause of a possible allergic reaction on the skin. This reaction is called allergic contact dermatitis.
Patch tests detect the type of allergy which is due to direct skin contact with things outside the body. It does not detect allergies related to diet or inhalation which might produce sneezing, asthma or hives.
This investigation allows for the identification of common chemicals and molecules that cause allergic contact dermatitis. We use the European Standard Battery of 36 individual chemicals.
Patches are applied usually on the upper back and must be kept dry.
This investigation will not identify less common contact allergies and these tests do require an experienced Dermatologist to interpret their significance. Testing for rare contact allergies is often limited to supra-specialist NHS Dermatology units.
The substances to be tested will be applied in small containers to your back and the sites marked with ink. The patches are stuck on your back and do not involve any injections. The patches stay in place for two days and are removed on the second visit when initial results are taken. The sites may itch, this is normal. More patches may be put on your back at this stage.
It may be necessary to expose part of your back to ultraviolet light if we suspect a light-induced contact allergy (‘Photopatch testing’). The final results are read on the third visit and the doctor will talk to you about them. The second and third visits should take no longer than half an hour. It is advisable to bring a book.
It is possible that your patch tests will be negative. This is helpful since, as far as we can, we have eliminated contact allergy as a cause of your skin problem. Positive reactions become red and itchy at the test site and usually appear by the third reading, although they can occasionally take longer. If you do develop a late reaction, please contact us.
Sometimes substances may stain the skin, this is normal.
Before the tests
Please bring samples either in the original container or in screw top, airtight container clearly labelled to say what it is and your name.
Typically and excluding your initial consultation fee, a charge of £150 is invoiced on application of the patch tests and a further £130 at review of the patch tests at a follow-up consultation a few days later.
1st Appointment
Consultation
£250
2nd Appointment
Patch test put on
£200
3rd Appointment
Reading & Result
£160
About 2% of the UK population has it, but many fail to be correctly diagnosed. The condition runs in families. The scalp, elbows and knees are the commonest places on the skin affected with red, dry, scaly and thickened skin that looks unsightly.
Most cases of psoriasis are mild – but it still can cause personal psychological and social problems. Most cases can be treated with the correct topical preparation but severe disease may require regular tablet or injection treatment. Phototherapy is also a very popular management for psoriasis. Occasionally psoriasis can affect the joints and require additional medical management from a rheumatologist.
Psoriasis is characterized by patches of thick, red, inflamed skin and dry, silvery flakes of skin known as scales. Symptoms range in severity from barely noticeable to outbreaks of lesions that cover most of the body, and psoriasis even causes a form of arthritis in some people. The condition is not contagious, so it cannot spread from person to person. A better understanding of psoriasis causes, symptoms, and treatment will help both afflicted and non-afflicted people cope with the physical and emotional challenges of living with the condition.

While the actual cause of psoriasis is unknown, it is believed to result from genes that influence the immune response in the skin, possibly causing areas in which the immune system is inadvertently directed against the body’s own cells. Some people have a genetic makeup that makes it more likely to develop psoriasis than others, and about one third of the people with psoriasis also have a family member with the condition. Psoriasis can flare up at any time without any apparent cause, but it is often initiated or aggravated by specific triggers. Some examples of triggers that may aggravate psoriasis symptoms are listed on your screen.
Researchers believe psoriasis results from inflammation and excessive skin cell production. In particular, T-cells, which are a particular type of white blood cell that aid the normal immune response, are activated unnecessarily. The T-cells are activated to such an extent that they influence a series of reactions that cause and maintain the inflammation while accelerating proliferation of skin cells. Skin cells normally take about a month to develop, mature, and move to the skin’s surface, where they are continually shed. During the heightened immune response that causes psoriasis, the skin cells mature in less than a week and move to the surface, where they accumulate, resulting in the formation of scales among the red, inflamed tissues.
Psoriasis can affect all age groups, but it primarily affects adults. About three-quarters of people with the condition develop it before the age of 40, and only about one in ten develop it in their childhood years. Males and females are affected about equally. Psoriasis is most common in people of northern European descent, varies among other ethnicities, and is rare in Native Americans. More than half of the psoriasis cases are mild, covering less than 3 percent of the body, with fewer moderate cases. Severe cases that cover more than 10 percent of the body are the least common. Although people may inherit the genes that make them more likely to develop the disease, they may or may not develop psoriasis due to a wide variability in triggers, environment, and personal health factors.
The inflamed, irritated areas – or lesions – linked with psoriasis are often associated with itching, pain and bleeding between the cracks in the skin around affected areas. The degree of itching and pain can vary from minimal to extreme, which may cause problems sleeping and carrying out everyday tasks. Psoriasis patches can occur anywhere on the body, but they are found predominantly on the scalp, face, back, elbows, palms, legs, knees, and soles of the feet. Psoriasis may also cause pitting, discoloration, and deformation of fingernails and toenails. In about one in ten people with psoriasis, inflammation in the joints causes symptoms of arthritis, which can affect them at any age.
There are five main types of psoriasis that are commonly identified. Plaque psoriasis is the most common and accounts for about 80 percent of psoriasis cases. People typically have only one of the five types at a time, but some of the types will occasionally occur together.
A dermatologist may take a small portion of skin, called a skin biopsy, for microscopic evaluation to help diagnose the type of psoriasis in order to determine the best treatment option. The variability in the disease means that each patient may respond to treatment differently, so a unique treatment may be chosen based on the type, location, severity of psoriasis, and medical history. In general, treatments fall into one of four general categories shown. Antibiotics are also used against secondary infections that may occur in open skin lesions. There is no cure for psoriasis, but the right combination of avoiding triggers and the correct use of a wide variety of treatment options may help alleviate symptoms between outbreaks.
South West Dermatology are able to offer biological treatment for psoriasis. Dr. Anthony Downs has over 20 years experience in prescribing biologics for patients with moderate to severe psoriasis.
If you feel this is the type of medication for you, then book in a consultation with Dr Anthony Downs. For patients outside the south west area Dr Downs is able to offer remote video consultations.
Biologics for psoriasis preceptorship program, Dept Dermatolgy, Exeter 2009-13.
This program was clinical teaching program aimed and up-skilling UK Consultant Dermatologist not familiar with prescribing biologic agents in clinical practice.
Downs AMR. Overnight application of dovobet ointment is a highly effective treatment for resistant scalp psoriasis.
Acta Dermato-Venereol 2006; 86:66-67. Laws PM, Downs AMR et al. Practical experience of ustekinumab in the treatment of psoriasis: experience from a multicentre, retrospective case cohort study across the UK & Ireland. Br J Dermatol 2012; 166:189-95.
Downs AMR Topical immunomodulators in dermatology. Pulse July 2005
Downs AMR Psoriasis – the scale of the problem. Chemist & Druggist Feb 2006
Downs AMR The use of biologics for psoriasis in a district general hospital. Dermatology in Practice 2007;15:8-10
Downs AMR Biologics in chronic psoriasis MIMS Winter 2008
Downs AMR, Dunnill MGS. Exacerbation of psoriasis induced by interferon-alpha treatment for hepititis C. Clin Exp Dermatol 2000; 25: 351-52.
Downs AMR. Etanercept vs. Adalimumab in the treatment of psoriasis Clin Exp Dermatol 2007; 32:593.
Downs AMR. Switching between anti-tumour necrosis factor biologic agents - is patient weight an important consideration? Brit J Dermatol 2009; 160:1123-24.
Downs AMR. Observational case series on a group of psoriasis patients who failed to respond to anti TNF alpha biologics and switched to ustekinumab. Brit J Dermatol 2010; 163:433-44
Bewley A, Boorman J, Cliff S, Domanne E, Downs AMR, et al. Interim results from a UK real world study to assess the impact of treatment with adalimumab on the physical and psychological manifestations and quality of life in patients with psoriasis. EADV, Istanbul 2013
Downs AMR, Bower CP. Psoriasis integrated care clinics: a novel approach to healthcare delivery. EADV, Istanbul 2013.
Bewley A, Boorman J, Cliff S, Domanne E, Downs AMR, et al. Results from a UK real world study to assess the impact of treatment with adalimumab on the physical and psychological manifestations and quality of life in patients with psoriasis. AAD San Fransisco 2015
Downs AMR. Scalp psoriasis. Korean Society of Dermatologists May 2010
Downs AMR. Integrated Care Clinics in psoriasis. NAPC Commissioning Conference London June 2011
Downs AMR. The Touch program interim data: improving compliance in psoriasis. 3rd World psoriasis and psoriatic arthritis conference Stockholm 2012.
Downs AMR. Managing scalp psoriasis Kuala Lumpor. Malaysian Dermatology Society May 2013
Downs AMR. Coping with Psoriasis – Patient/Physician challenges and the role of Emollients in psoriasis. Dubai 2103
Downs AMR, Biologics for severe psoriasis. Amman, Jordanian Dermatology Society September 2014
Williams P, Savanovic-Abel O, Haigh R, Winfield W, Batchelor R, Downs A. Successful treatment of Dermatomyositis-Associated Calcinosis with Adalimumab. Clin Exp Derm 2016.
Our Consultant Dermatologist have been managing psoriasis since 2000. We offer the management of all types of psoriasis and related conditions.

