The South West’s premier independent dermatology & skin clinic

Nearly one in ten people worldwide will develop eczema — a term that describes skin conditions characterized by irritated, inflamed, itchy patches. Eczema is also called dermatitis, and the two terms are often used interchangeably. In some people, eczema causes the skin to appear very red with a rash that seems to bubble up; in others it can appear scaly and dry with less discoloration. Eczema often appears after an itch has been scratched, and therefore is commonly referred to as “the itch that rashes.” In this animation you will learn about the way eczema occurs and what triggers it, different types of eczema, and how you can manage your eczema and possibly prevent future outbreaks.

The skin is composed of two layers: the epidermis and the dermis. The epidermis is the outer layer that acts as the body’s primary defense against the environment. The dermis, or innermost layer, is responsible for providing structure and support to the skin. Eczema is believed to arise when the body’s immune system is triggered into an abnormal, overactive, inflammatory response that involves both the epidermis and the dermis. Another theory suggests that in some cases a defective epidermis causes an individual to be particularly sensitive to substances that cause an inflammatory response. The inflammation that results from eczema irritates patches of skin, causing them to itch. Regions of elevated, fluid-filled bumps may also develop. With continued scratching these bumps may burst and exude pus and become crusty, or the skin may become dry and cracked. Although eczema is not commonly associated with life-threatening risks, if scratching causes any openings through the skin that penetrate into the dermis, the skin may become infected.
Click to watch video (video will open in a new window)
Eczema occurs at any age and tends to arise in certain body areas more than others, depending on age. For example, in infants, eczema typically appears on the forehead, cheeks, forearms, legs, scalp, and neck. In contrast, children and adults most commonly experience patches of eczema on the face, neck, upper chest, elbow creases, wrists, hands, fingers, back of the knees, ankles, and feet. However, it is important to realize that eczema can occur on any part of the body at any age. Depending on the cause and type of eczema, it can spread over large areas of the body, or it may be confined to a specific region, as in cases where the eczema is triggered by contact with a particular substance. Eczema can also be associated with asthma and hayfever. Fillagrin gene mutation allows for the skin water barrier to be less efficient. This causes excessive skin dryness and soreness leading to skin inflammation (dermatitis). The immune system tends to respond in a different way to normal which compounds the situation. Allowing the skin to dry out, skin infection and (very rarely diet) can cause flares of eczema.
Although dermatologists do not fully understand the exact cause of all eczema, they have identified a variety of potential sources. Some people may have a genetic predisposition because eczema tends to be more common in people whose family members have allergies, asthma, or eczema. In others, eczema may result from a variety of factors known to trigger eczema flare-ups, which include the following categories and the examples shown on your screen.
The most common type of eczema is known as atopic eczema. Ten to twenty percent of infants in the United States are affected by atopic dermatitis. Although atopic dermatitis usually occurs before the age of five, it can appear for the first time, or reappear periodically, at any age. This type of dermatitis is believed to result from an interaction of genes, the environment, the way the epidermis renews itself in particular individuals, and an overactive immune system. Most affected individuals have a family history of allergies and one or two parents who have experienced eczema in the past.
Substances absorbed through the skin can lead to the development of allergic contact dermatitis. The skin often feels sore rather than itchy. Those with atopic dermatitis are more vulnerable to develop this problem. Common causes include Nickel, Chrome, Cobalt, Perfume, PPD and Colophony. Allergy ‘patch’ testing can confirm the causative chemical or substance.
Contact dermatitis occurs when a substance that causes an inflammatory response touches the skin. There are two primary forms of contact dermatitis known as irritant contact dermatitis and allergic contact dermatitis. Substances that irritate the skin, such as a chemical or a particular type of soap, cause irritant contact dermatitis. This form generally requires contact with a certain threshold amount of the irritating substance before symptoms develop. After contact with this threshold amount, the skin gradually starts to react and a rash typically develops in the exposed area. Allergic contact dermatitis arises after exposure to an allergen, such as poison ivy. Even small amounts of the allergen can trigger a response in susceptible individuals. Unlike irritant contact dermatitis, the body’s immune system may overreact in response to the allergen, which can cause inflammation to spread to areas of the body that didn’t actually contact the substance.
Skin can dry out and become sore if exposed to irritants. The skin then becomes more sensitive – even to minor irritants. People with atopic dermatitis are more vulnerable to this problem.
Although there is no real cure for eczema, symptoms can often be reduced or prevented by avoiding specific triggers, such as those shown on your screen. The most effective measure you can take to clear an eczema flare-up is to avoid the urge to scratch the affected area, as this may worsens outbreaks. To avoid further irritation, keep your fingernails short and smooth. Bathing in lukewarm water, using special cleansers, and applying moisturizers directly after bathing are also often effective in clearing symptoms. Other common treatments are shown on your screen. In the severe cases where other treatments have failed to work, medications that affect the body’s immune response may be recommended.
Contact dermatitis symptoms generally subside after removing the source. This process may take several weeks to clear, but can often be shortened to days with treatment. Oral medications prescribed for severe cases can be quite effective and have few side effects when taken for a short duration. About half of the atopic eczema cases in infants clear by a year and a half to two years of age, while others take longer or may never completely disappear. A person may continue to exhibit signs into adulthood, primarily as eczema on the hands. When treated, atopic eczema can be stubborn and is prone to recurring outbreaks. You may need to adjust how you use medications, switch to stronger medications, or even reduce your stress level by taking more time for relaxing activities. Fortunately, the therapies available today are often effective, and with proper treatment and prevention, most eczema can be controlled or even alleviated.
Often looking like a nettle rash or bee stings. Very itchy and flares are random and spontaneous. Sometimes aggravated by pressure on the skin, changes in temperature, sweating, water exposure, certain drugs or certain chemicals in the food. The problem is an immune defect (not an allergy) causing histamine release in the skin. An associated condition called angioedema can cause skin swelling especially of the lip or tongue.
Publications in Eczema, Urticaria and Allergy
Downs AMR, Sansom JE. Palmo-plantar dermatitis may be due to phenol formaldehyde resin contact dermatitis. Contact Dermatitis 1998; 39:147
Downs AMR, Lear JT, Sansom JE. Contact sensitivity in patients with oral symptoms. Contact Dermatitis 1998; 39:258-9
Downs AMR, Sharp LA, Sansom JE. Pentaerythritol esterified gum rosin as a sensitizor in Granuflex hydrocolloid dressing. Contact Dermatitis 1999; 41:162-3
Lotery H, Kirk S, Beck M, Bovera E, Crone M, Curly R, Downs AMR et al Dicapryyl maleate: an emerging cosmetic allergen. Contact Dermatitis 2007; 57:169-72.
Downs AMR, Fifield R, Sansom JE. IgG latex RAST is not a specific marker for type I hypersensitivity. Contact Dermatitis 1999; 41:223-4.
Downs AMR, Sansom JE. Colophony allergy - a review. Contact Dermatitis 1999; 41:305-10.
Downs AMR Topical immunomodulators in dermatology. Pulse July 2005
Bugowski P, Downs AMR Eczema, a treatment overview. www.doctors.org August 2012
Downs AMR, Kennedy CTC. A case of palmo-plantar pruritus responding to ondansetron. Arch Derm 1998; 134:925-6.
Downs AMR, Sansom JE, Simmons I. Let Rip! Fun Pot dermatitis. Contact Dermatitis 1998; 38:234.
Downs AMR, Lear JT, Kennedy CTC. A case of triamcinolone anaphylaxis. Arch Derm 1998; 134:1163-4
Downs AMR, Sansom JE. Occupational contact dermatitis to propolis. Contact Dermatitis 1998; 38:359-60.
Downs AMR, Lear JT, Wallington TB, Sansom JE. Contact sensitivity and systemic reaction to pseudoephedrine and lignocaine. Contact Dermatitis 1998; 39:33.
Downs AMR, Sansom JE. Airborne occupational contact dermatitis from epoxy resin in an immersion oil used in microscopy. Contact Dermatitis 1998; 39:267.
Downs AMR, Sansom JE. Severe contact allergy to footwear responding to handmade shoes. Contact Dermatitis 1999; 40:218.
Downs AMR, Lear JT, Dunnill MGS. Polymorphic light eruption confined to vitiligo. Clin Exp Derm 1999; 24:79-81.
Downs AMR, Kirkup M. The dangers of body painting. BMJ 1997; 315:1722.
Condon CA, Downs AMR, Archer CB. Terbinafine induced acute generalised exanthematous pustulosis. Br J Derm 1997; 138:709-10.
Downs AMR, Kennedy CTC. Somatrophin-induced acanthosis nigricans. Br J Derm 1999; 141:390-1.
Downs AMR, Kennedy CTC. The anti-pruritic effects of ondansetron. Arch Derm 1999; 135:599.
Kirkup ME, Downs AMR, Sansom JE. Does 5% doxepin cream affect patch test reactions? Br J Dermatol 2003; 148:847.
Downs AMR, Sansom JE. A retrospective assessment of colophony positive patients. 5th Congress of the European Society of Contact Dermatitis, Amsterdam, 2000.
Kirkup ME, Downs AMR, Unswoth JO, Sansom JE. Experience with tranexamic acid for non-hereditary angio-oedema and urticaria. BAD, Brighton 2003.
Bowling JCR, Scarbrick J, Warin AP, Downs AMR. Multicomponent hair dyes, hidden causes of allergic contact dermatitis. BAD, Brighton 2003
Bogucki P, Downs AMR, Interstitial granulomatous drug reaction (IGDR) triggered by infusion of eryrthomycin used as a sclerosing agent. EADV, Prague 2012
Bogucki P, Downs AMR. Erythema multiforme during treatment with IL-12 & IL-23 inhibitor. AAD, Miami 2013
Downs AMR, Charman CR, Lewis V. Integrated care approach to eczema: presentation of service data and potential quality measures from a community pilot clinic. EADV, Istanbul 2013
Ling GS, Downs AMR. Occupational airborne allergic contact dermatitis to usnic acid in an office-based dentist. AAD San Diego 2018.
Our consultants dermatologist have been managing eczema, urticarial and a wide variety of skin rashes as a consultant dermatologist since 2000.
We offer the management of all types of eczema/dermatitis, drug rashes & urticaria including patch tests for allergic contact dermatitis and blood tests for Type 1 allergies.
Between ten and twenty percent of people worldwide develop atopic dermatitis — a term that is sometimes used interchangeably with eczema to describe skin conditions characterized by irritated, inflamed, itchy patches. People who have atopic dermatitis have long-lasting dermatitis symptoms, and they often have a history of allergies, asthma, and one or more family members who have experienced atopic dermatitis. In some people, atopic dermatitis causes the skin to appear very red with a rash that seems to bubble up; in others it can appear scaly, flaky, and dry with less discoloration. Atopic dermatitis is not contagious and is believed to result from genetic factors that influence the function of the skin, causing it to be extra sensitive to irritants.
Your skin is composed of two main regions: the epidermis and the dermis. The epidermis is the outer layer that acts as the body’s primary defense against the environment. It keeps out germs and allergens, which are substances to which the body produces an allergic response. The dermis lies beneath the epidermis and is responsible for providing structure and support to the skin. On most of the body, the epidermis is actually comprised of four distinct layers as shown. Cells produced in the stratum basale are pushed outward as new cells develop, and they gradually die as they migrate to the stratum corneum at the surface where they eventually slough off. Normally, the rate of skin production and loss are equal so that the thickness of this outer layer remains constant. However, in some instances more skin cells may be shed from the stratum corneum than accumulate or excessive skin cells may accumulate as abnormally thickened skin.
Atopic dermatitis is believed to result from how a person’s genes influence their immune response and formation of the epidermis. Researchers don’t know the exact cause, but there are two primary theories. In one, it is believed that genetic factors influence the immune system in the skin, causing it to react as if a person has contacted something to which they are allergic. A series of internal reactions cause itchiness and inflammation that damages the skin’s barrier layer (stratum corneum). The damage results in increased water loss through the epidermis, resulting in dry patches and further degradation. Allergens and germs may enter the eroded skin, setting off more reactions. In another theory, it is believed that a person’s genes cause the outer layer (stratum corneum) of skin to be abnormal and ineffective as a barrier. Excessive water is lost through the skin, causing dryness and a breakdown of the outer layer. Allergens and germs are able to penetrate, starting a cycle of itchiness and inflammation that further erodes the skin.
The majority of patients with atopic dermatitis have regions that are constantly itchy, even when there are no other symptoms. When inflammation develops from atopic dermatitis, it irritates patches of skin, causing them to redden and become so itchy that it is hard to resist scratching. Regions of elevated, fluid-filled bumps may potentially develop. With continued irritation, these bumps may burst and exude pus and become crusty, or the skin may become dry and cracked. Although atopic dermatitis is not commonly associated with life-threatening risks, if scratching the itch causes openings through the skin that penetrate into the dermis, germs may enter and cause a secondary infection. In some people, the skin responds to continued, long-term scratching of itchy areas by producing an excessively thick outer layer. This process, which is called lichenification, results in the skin having a leathery, cracked appearance.
The majority of cases of atopic dermatitis begin during the first year of life, and about ninety percent of cases first occur before age five. Although it is rare, atopic dermatitis can also first occur at the onset of puberty or later during adulthood. Active atopic dermatitis can disappear entirely, or it may enter a period of remission and recur as a flare-up at some point in the future. About half of the atopic dermatitis cases in infants clear by a year and a half to two years of age, while others take longer or may never completely disappear. A person may continue to exhibit signs into adulthood, primarily on the hands, and symptoms elsewhere can recur periodically at any age.
In infants, atopic dermatitis typically appears on the scalp, forehead, cheeks, neck, forearms, and legs. In contrast, children and adults most commonly experience patches of atopic dermatitis on the face, neck, upper chest, elbow creases, wrists, hands, fingers, back of the knees, ankles, and feet. Although there are tendencies, atopic dermatitis can occur on any part of the body at any age, and it may be triggered by a variety of irritants that vary from person to person. These irritants include dry skin, sudden temperature changes, abrasive fabrics, certain chemicals and smoke, various food items, substances from living organisms, and environmental factors as shown. Sometimes triggers can be identified with skin allergy tests, but often they are difficult to determine and are only identified after observing changes in one’s diet or the products one uses and noting when and how symptoms worsen or improve over time.
There is no cure for atopic dermatitis, but it can often be managed with treatment, avoiding triggers, and taking preventative actions. Keeping fingernails short and resisting the urge to scratch can also prevent making conditions worse. Sleeping in hand mitts may help children, who find it particularly difficult to resist scratching. Bathing in lukewarm water, using special soaps, and applying moisturizers directly after bathing are also often effective in clearing symptoms. New products designed to limit water loss and improve the structure of the skin barrier are also effective in many patients. Although not always necessary, the primary medications used for treating atopic dermatitis include moisturizers, which reduce dryness; corticosteroids, which reduce swelling and reduce itchiness; immune modulators, which suppress the skin’s immune response; and antihistamines, which reduce itchiness.
Fortunately, a childhood onset of atopic dermatitis will usually resolve naturally over time. In people with persistent or recurring symptoms, available treatment options can help control atopic dermatitis. Consulting a health care provider can help you more rapidly identify triggers, manage the symptoms of flare-ups, and find the best treatment option for your particular skin. Although there is no cure, symptoms can usually be managed well enough to lead a comfortable, productive life.
Affected areas may also be reddened, inflamed, and cause an itching or burning sensation. A mild form of seborrheic dermatitis on the scalp is one cause of dandruff. Seborrheic dermatitis is not contagious, meaning it cannot be acquired through contact with a person who has this skin condition. This animation will describe the possible causes of seborrheic dermatitis, how and where this skin condition occurs, and options that are available to treat it.
To understand how seborrheic dermatitis occurs, it is important to understand some of the basic anatomy of your skin. Your skin is composed of two layers, known as the epidermis and the dermis. The epidermis serves as your skin’s primary defense against the environment. The dermis provides your skin with structure, support, and elasticity. Sebaceous glands are found within the dermis, typically near hair follicles, although they can occur in hairless areas as well. These glands secrete an oily substance known as sebum, which lubricates the surface of your skin and prevents it from drying out.
The exact cause of seborrheic dermatitis is unknown. One theory proposes that seborrheic dermatitis is a reaction to particular types of yeast (Malassezia genus), which are single-celled organisms that are commonly found on human skin. Typically, the yeast cause no problems, but in some people when the yeast metabolize sebum, they generate byproducts that irritate the skin. Another theory, which complements the yeast theory, suggests that seborrheic dermatitis may result from excessive sebum production. Yeast are found in sebum rich areas and may be more likely to cause skin irritation in areas of the skin that produce excessive sebum. An additional factor believed to be linked to seborrheic dermatitis is an increased level of the hormones known as androgens, which control sebaceous gland activity. Seborrheic dermatitis is more frequent in males, who produce more androgens than females, temporarily in infants who have been exposed to high androgen levels in the womb, and following puberty, when androgen levels increase in both sexes.
Seborrheic dermatitis usually occurs after puberty, affecting people between the ages of 20 and 50, although it can also occur in infants. In infants this condition has been termed “cradle cap”, since it typically affects the scalp, and it usually disappears spontaneously by six months to one year of age. Seborrheic dermatitis arises most frequently in males and in persons affected by a central nervous system disorder, such as major paralysis or Parkinson’s disease. Seborrheic dermatitis primarily affects areas of the skin that have the most numerous and active sebaceous glands. These areas include the scalp, hairline, eyebrows, eyelashes, creases of the nose, external ear canal, skin behind the ears, and areas along skin folds of the trunk, such as the armpits, navel, groin, and buttocks. In infants, in addition to “cradle cap” on the scalp, seborrheic dermatitis can also affect the face and diaper area.
In most cases of mild seborrheic dermatitis, cleansing daily with an anti-dandruff shampoo is recommended. Washing the affected areas with a mild soap or soapless cleanser may also help decrease surface sebum. If symptoms persist despite daily cleansing, additional treatment options are available, including anti-fungal medications used to control the growth of yeast and anti-inflammatory medications used to reduce redness and inflammation. Lotions and creams containing ingredients such as coal tar, corticosteroids, salicylic acid, selenium, sulfur products, and zinc may be advised to clear more persistent scales. In addition, some people notice that sunlight exposure improves their symptoms.
Although there is no cure, the symptoms of seborrheic dermatitis can usually be managed successfully, allowing people to lead comfortable, productive lives. Several treatment options are available, and finding the right treatment to fit your specific needs may take time. It is suggested that you begin with mild treatments and switch to more intensive treatments if necessary. Consulting a health care provider can help you identify the best treatment option for your particular skin and seborrheic dermatitis symptoms.
Nearly all individuals during their teen years are affected to some extent by acne. Acne even affects some people well into adulthood, making it the most common type of skin condition. Acne affects both men and women and most commonly occurs on the face, neck, back, chest and upper arms. Although it is generally not considered a serious health condition, it may cause embarrassment and even scarring of the skin in severe cases. Even if you are affected by severe acne, there is good news! There are a variety of different treatment options available to treat acne that will help restore a smooth, healthy glow to your skin.
Before you learn how best to treat your acne, it is important that you understand the basics of your skin’s anatomy and how acne occurs. Your skin is composed of two layers known as the epidermis and the dermis. The epidermis is the skin’s primary defense against the environment. The dermis is primarily composed of collagen and elastin fibers, which provide the skin with structure, support, and elasticity. Blood vessels and nerves run throughout the dermis. The blood vessels transport blood, which supplies important nutrients to your skin and the nerves allow you to perceive sensations like pain, temperature, and touch. Your skin has many pores, which are actually small openings in the skin from sweat glands, hair follicles, and sebaceous glands deep within the dermis.
Acne results from clogged pores. What you may not know is acne generally occurs in sebaceous glands that are attached to hair follicles—not sweat glands. The greatest number of sebaceous glands is found on the face, neck, and back, which is why acne commonly occurs in these regions. Sebaceous glands are special glands attached to the hair follicle. Together, the hair follicle and sebaceous gland are often referred to as the pilosebaceous follicle. Sebaceous glands produce an oily substance known as sebum, which helps make your skin waterproof and prevents it from drying out.
You have probably heard that things like chocolate, soda, and greasy foods like pizza can cause acne. While this may be true for very select individuals, physicians do not generally believe this to be the case. Acne is usually caused by a combination of factors including a build up of dead skin cells, excessive sebum production, and bacterial overgrowth. As these factors become more severe, so too does the acne. What starts out as mild acne may progress into moderate or severe acne, depending on the conditions in your skin. Let’s take a look at how these different stages of acne develop.

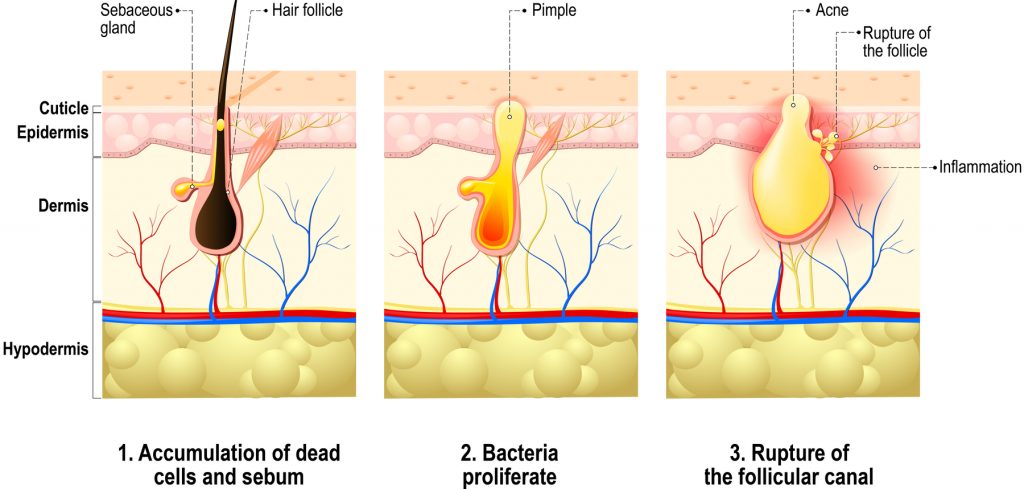
Dead skin cells are continuously shed from the walls of hair follicles during a process known as keratinization. Under normal circumstances, the skin cells do not build up and the sebum is secreted onto the skin’s surface. However special conditions can promote an increase in keratinization. If too many skin cells build up in the follicle, they may actually block the secretion of sebum, which causes a plug to form. This plug is what is commonly known as a blackhead or a whitehead, which are mild forms of acne. Blackheads generally appear as small, black holes on the skin’s surface. When the follicle is not completely blocked, it opens slightly and the top of the plug turns black, which is what you see as a blackhead. In contrast, whiteheads generally appear as small, skin-colored bumps beneath the skin’s surface. The follicle opening is completely blocked with sebum and dead skin cells, which is what you see as a whitehead.
Acne formation gets even more complex. In response to hormones known as androgens, like progesterone and testosterone, the sebaceous glands produce more sebum. This is why acne usually starts to occur during puberty and why women may experience more acne at the onset of menstruation. When excess sebum is produced in already blocked pores the follicle becomes inflamed. Further inflammation can be caused by bacterial overgrowth as well. Together, this causes a papule to form, which is a red, raised bump on the skin.
Continual sebum production and bacterial overgrowth increase the inflammation around the follicle even further. Like a dam that cannot hold any more water, the follicle may eventually rupture, spilling its contents into the skin layers below. When this happens, pustules form. This is because your body sends white blood cells to the area as an immune response. These white blood cells along with other debris create pus, which is what gives pimples their white or yellowish center.
In cases in which inflammation becomes even more severe, nodules and cysts may develop. Nodules are large, round bumps that originate deep beneath the skin’s surface. They are typically caused by severe inflammation and infection within the dermis. Although similar to nodules, cysts are usually filled with pus. Both of these types of acne may be long lasting and painful. In addition, nodules and cysts may lead to acne scarring and generally only respond to intense forms of treatment.
Antibiotic treatment has been a standard approach in treating acne for many years. Available in both topical and oral formulas, antibiotics such as erythromycin and tetracycline are often used to treat moderate to severe acne. Antibiotic treatment works by reducing acne-causing bacteria, sometimes by as much as ninety percent. However, unlike benzoyl peroxide, antibiotics work to reduce inflammation as well. This is why dermatologists often combine topical antibiotics with benzoyl peroxide for better results. Your dermatologist may start you off with a high dosage and gradually decrease it as your acne improves over the course of several months. It is important to realize that if you use the same antibiotic treatment for a long period of time the bacteria may eventually develop resistance, which means that the treatment will stop working. However, under these circumstances, different antibiotics can usually be used.
Certain oral contraceptives, or “the pill,” have been found to be effective in treating acne in women. As you learned earlier, sebaceous glands produce more sebum in response to androgens, which promotes acne formation. Oral contraceptives work by reducing androgens. As a result, sebum production decreases, which reduces acne. Oral contraceptives can be used over a long period of time to treat your acne, although it may take a few months for you to notice an improvement in your complexion. It is important to realize that if you stop taking the pill, your acne may return. Although there are many different forms of the pill, not all of them can be used to treat acne. You should discuss the different options with your physician to find the treatment that is right for you.
Clascoterone cream has been available in the USA & Canada for over two years and has rapidly become a popular treatment. It is an androgen receptor inhibitor without any systemic absorption and so suitable for men and women. Clascoterone reduces oil (sebum) production and inflammation. It takes time to work – anywhere between 12 to 24 weeks. It is well tolerated and only causes mild skin irritation, redness and dryness.
Retinoids are Vitamin A derivatives and are available in topical and oral formulas. Commonly used to treat mild to moderate acne, topical retinoids work by unclogging your pores and also preventing new whiteheads and blackheads from forming. Like other acne treatments, topical retinoids can increase the effectiveness of benzoyl peroxide and antibiotics when used together. In contrast to topical retinoids, oral retinoids are only appropriate for the most severe cases of nodulocystic acne. They work by reducing sebum production, limiting the build up of dead skin cells, inhibiting the growth of acne-causing bacteria, and even reducing redness and inflammation. While oral retinoids can produce significant results, they also come with serious side effects such as increased cholesterol, compromised digestive and liver function, and even birth defects. Therefore, you should discuss your health history as well as the possible side effects with your dermatologist to determine if the treatment is right for you.
If individual spots last more than 10 days then there is a high risk of that person eventually developing acne scars. Scars may be ice-pick, hypertrophic or atrophic. Certain topical anti-acne products may limit the development of scars. Scars can be improved but not eliminated by a range of dermatological treatments.
Acne can cause marks especially in non-white skin. These can last for many years before fading - but some never fade away. Treatments are available to help remove these marks and prevent them happening.
The light emitted from Ipulse helps to destroy the bacteria which causes acne by exciting the existing oxygen molcules and increasing the molecules power. These super powered molecules break down the bacteria that cause acne and create an atmosphere where it cannot breathe. By boosing the skin’s internal cleansing system in this way, Ipulse dramatically reduces acne and the occurrence and apperance of scarring, resulting in much clearer skin.
IPL is a recognised treatment for mild to moderate acne. It calms overactive grease glands and removes bacterial infection – particularly when used with specialist skin care.
How does IPL work?
A powerful beam of ordinary light is released as a single or series of short pulses. The light destroys bacteria and shrinks grease glands within the skin. Both are necessary to form acne spots.
How is the treatment carried out?
You will be asked to put on some goggles to protect your eyes. A layer of chilled gel is applied to the area to cool the skin during treatment. A pulse of light is delivered into the skin which last for less than a second. A feeling of warmth or skin pricking is felt with each pulse of light. About 50 pulses may be required to treat the whole face.
Am I suitable for treatment?
Dark-skin or sun-tanned skin (including fake tan) cannot be treated. All make-up must be removed. Certain skin or medical conditions, skin treatments and medicines may exclude a person from treatment. The beard area in men may suffer from permanent hair loss.
Is it safe?
The area is usually red immediately after treatment. This settles in a few hours. Blistering may occur if the light pulse is set too strong or if make-up is left on the, or if the skin is too dark or sun-tanned. This may lead to discoloration of the skin.
How long does each treatment last?
A treatment session can last about 15 minutes.
Glycolic acid peels, topical anti-acne prescription medications and photodynamic therapy can be combined with IPL to maximise results.
How many treatments are necessary?
Typically a course of six IPL treatments with each treatment every 2 weeks are needed. Glycolic acid peels can be done in the alternate weeks.
Consultation procedure
There are a variety of skin complaints that look like acne and types of acne that are not suitable for IPL.
A consultation with a consultant dermatologists* is advised to correctly diagnose your problem, estimate the success of IPL for you and discuss a well as offer the full range of alternative medical treatments available.
Aftercare
Sun tanning after IPL treatment will delay further treatment until it has settled and may cause temporary skin darkening.
*Member of the Royal College of Physicians and Member of the British Association of Dermatologist
Dr Anthony Downs, consultant dermatologist has been managing acne with a variety of patients since 2000. Dr Downs can help you diagnose and treat acne with a bespoke treatment designed to your individual needs.
Mr Downs can offer topical and oral treatments for active acne including isotretinoin, management of acne cysts including steroid injections, removal of post-inflammatory dark marks with topical treatments or lasers and the improvement of all types of acne scars with topical treatments, surgery, steroid injections, vascular lasers and fractionating lasers.
Dr Downs has also been involved as a research collaborator in:
Acne national genetics clinical trial 2009-2014
Acne Publications
With so many choices available for patients, it can seem overwhelming to decide who can offer the best advice, the safest treatments and the most dependable outcome. Television, magazines, and other media can give misleading information to patients who are curious about the latest products and procedures.
Intense Pulsed Light
For the treatment of red thread veins, acne, unwanted hair, sun-damaged skin, photo rejuvenation, red & brown blotchy skin and age spots. Also used as an alternative to laser therapy where this has failed to work sufficiently well.
Treatments for lines and wrinkles
Treatments for localised excess sweating
Soft tissue fillers
For volume loss and to smooth out wrinkles.
Porphyrins are naturally occurring chemicals that when exposed to light glow or burn. This phenomenon has been exploited to successfully treat many different kinds of cancer.
Liquid nitrogen treatment for viral warts and other superficial blemishes.
For the accurate assessment of moles. This technique confidently diagnoses harmless skin blemishes from skin cancers including melanoma. This avoids unnecessary surgery and allows for long-term mole monitoring in those at risk from developing skin cancer, particularly melanoma.
The removal under local anaesthetic in a modern skin surgical unit of harmless but annoying skin lesions and skin cancer.
Assessment of immediate and delayed allergic reactions. RAST tests, food battery and inhalation battery screens, and patch testing.
Microsclerotherapy is a technique that enables removal of unsightly thread veins that commonly occur on the legs in women. It involves injection of a chemical known as a ‘sclerosant’ in to the vein through a tiny needle and is usually painless. Up to 20 or 30 veins can be treated in one session which lasts around 45 minutes. A course of 3 – 5 treatments is commonly required, spaced at around 4 weeks apart.
Patients are advised to mobilise normally following injection and we recommend wearing some form of compression hosiery after treatment to reduce potential bruising and swelling.
Around 80% of veins treated are permanently removed although other veins may develop as time goes on. Occasionally patients experience some discomfort after treatment and a rare complication is inflammation and ulceration of the skin overlying the treated vein.

